
Louisiana Food As Medicine NOGO, Maine puts $30M out for EMRs
Virginia deep dive: where “VA Rural Vitality” stands as of today

Don’t sleep on last week’s data dumps:
2026 Q2 Newsletter Activity Index: state-by state, topic-by-topic deeplinks
Q2 RFP Review / Q3 RFP Watcher: Every procurement from Q2, near-term contracting outlook, and state-by-state analysis
The 50-State RHTP Field Guide: downloadable PDF with RHT personality, program maturity, federal outlays, open procurements, engagement activity, rural geography, and contacts
In this issue:
Ohio closes the loop: $10M workforce award lands at Ohio University
Virginia Implementation: The “VA Rural Vitality” Framework
Louisiana out with Food As Medicine NOFO
Maine to put $30M out for EMRs — and nobody has to compete for it
Ohio closes the loop: $10M workforce award lands at Ohio University
Ohio University has been awarded the full $10 million offered under DOH59715, the Ohio Department of Health’s rural workforce pipeline solicitation — 100% federally funded by CMS/HHS, announced July 10, 2026.
What the money buys is a convening structure, not a program. OHIO will lead Health Workforce Ohio, a statewide strategy co-led by The Health Collaborative and steered by the Ohio Association of Community Health Centers, which chairs an 11-organization steering committee. More than 85 organizations across health care, education, and workforce are lined up as partners. The stated work is career-exploration pipelines for students, apprenticeships and work-based learning, telehealth and digital-health training, and upskilling the incumbent workforce — concentrated on nursing, behavioral health, allied health, and community-based care.
Why it matters
Watch the governance shape, because other states will copy it: a university as fiscal and convening lead, a primary care association chairing the steering committee, and a partner network large enough that the real procurement activity moves downstream of the state. Ohio’s $10M is now a subaward funnel, and OHIO is explicitly inviting employers, training institutions, and community partners to come find funding at healthworkforceohio.org. If you sell into rural workforce — training platforms, credentialing, placement, telehealth education — the buyer in Ohio is no longer ODH. It’s Athens.
Virginia Implementation: The “VA Rural Vitality” Framework
Virginia’s entry into the federal Rural Health Transformation (RHT) Program is branded “VA Rural Vitality,” a five-year strategic investment plan managed by the Department of Medical Assistance Services (DMAS).
Last week I added this new (to me) site to our nightly scrape based on an inquiry I received from a reader.
For the first budget period, Virginia secured a confirmed federal award of 189,544,888.14. The program focuses on 76 rural counties, collectively known as the “rural horseshoe,” which represent 57% of the Commonwealth’s total counties and approximately 1.5 million residents.
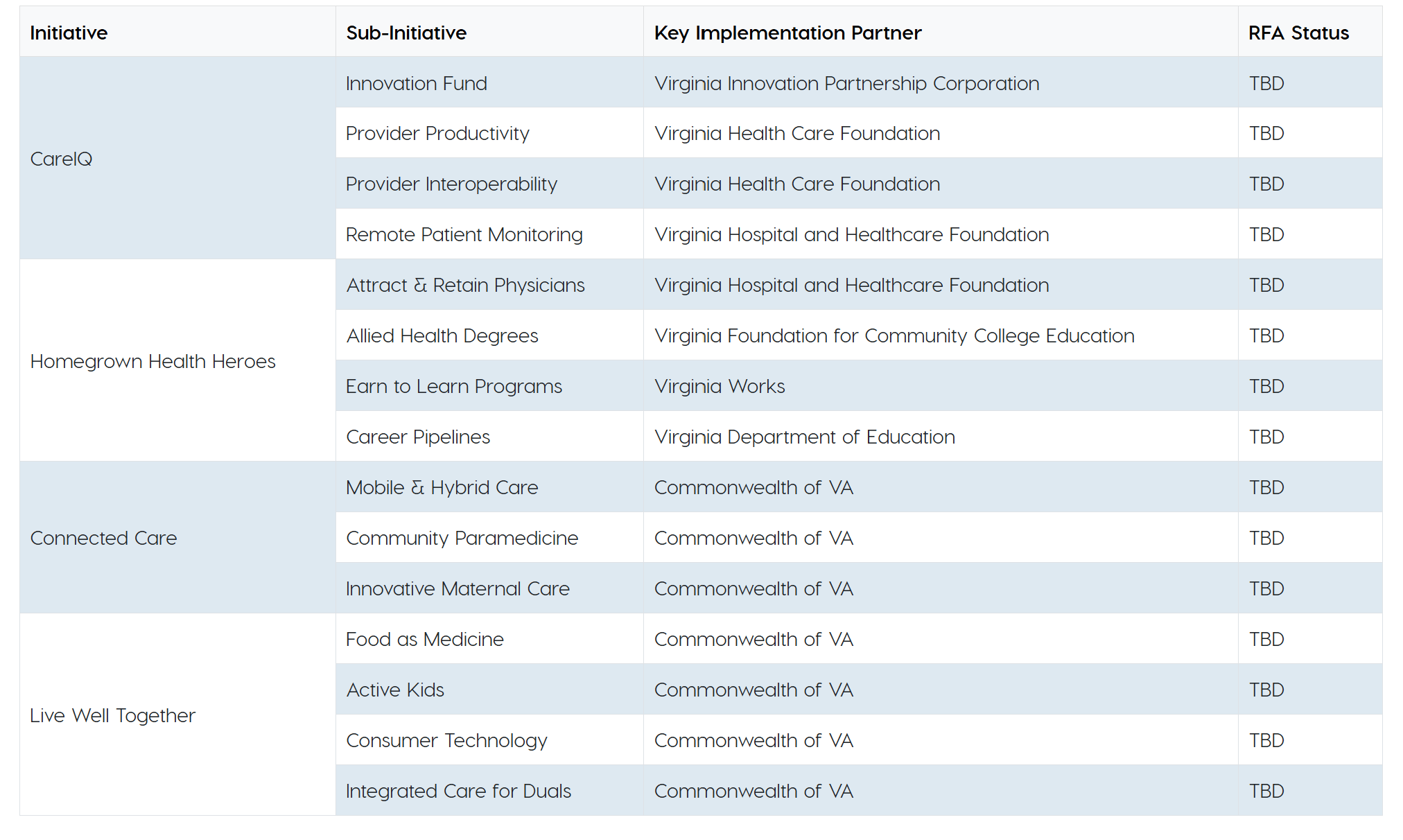
The Administrative Approach: A Partner-Led Model
Unlike some states managing the entire grant portfolio centrally, Virginia utilizes a named subrecipient model. DMAS acts as the lead state agency and primary recipient of the CMS cooperative agreement, providing oversight and ensuring federal compliance, but it delegates the actual administration of specific funding streams to “Key Implementation Partners”. These partners are responsible for releasing downstream Requests for Applications (RFAs) to local providers and organizations. As of mid-2026, the state is transitioning from Phase 1, where partners are already established and contracting, to Phase 2, which involves identifying administrators for its access and wellness initiatives.
Workforce Development: Homegrown Health Heroes
Proposed at $132.0 million over five years, this initiative is front-loaded as a Year 1 priority to address critical clinician shortages. It mandates a five-year rural service commitment for participants in its residency and apprenticeship programs.
Physician Residency: Administered by the Virginia Hospital Research and Education Foundation (VHREF), this sub-initiative aims to fund 80–100 residency slots in high-priority specialties like OB/GYN, Family Medicine, and Psychiatry.
Allied Health Degrees: The Virginia Foundation for Community College Education (VCCS Foundation) manages a “hub-and-spoke” model to expand enrollment in two-year health programs, utilizing mobile simulation labs to reach rural campuses.
Apprenticeships: Virginia Works administers “Earn to Learn” programs, targeting 1,500 new registered apprentice slots over the five-year period.
K-12 Pipelines: The Virginia Department of Education (VDOE) oversees high school health academies and Career and Technical Education (CTE) expansions to create job-ready pathways for roles like EMTs.
Tech Innovation: CareIQ
With a proposed budget of $282.6 million, CareIQ is designed to modernize rural legacy infrastructure.
Tech Innovation Fund: The Virginia Innovation Partnership Corporation (VIPC) administers a fund providing non-dilutive grants of up to $500,000 to Virginia-based health-tech startups developing solutions for rural chronic disease.
Interoperability and Productivity: The Virginia Health Care Foundation (VHCF) manages a fund to help FQHCs, free clinics, and rural hospitals modernize Electronic Health Record (EHR) systems and adopt AI-driven workflow tools.
Remote Patient Monitoring (RPM): VHREF oversees the deployment of wearables and clinical dashboards, allowing providers to track patient outcomes continuously in facility and home settings.
Access and Wellness: Phase 2 Initiatives
These initiatives focus on bringing care directly to residents rather than requiring travel to distant urban centers.
Connected Care, Closer to Home ($412.0M): This includes mobile health units, telehealth kiosks, and “Community Paramedicine” programs. The latter enables EMS providers to offer treat-in-place care and preventative home visits, leveraging an ET3-style payment model.
Live Well, Together ($124.2M): This focus area includes “Food as Medicine” (produce prescriptions and medically tailored meals) and “Active Kids,” which funds the minor renovation of underutilized community spaces for youth physical activity.
Spending and RFP Status
Virginia’s first-year obligation of $189.5 million must be fully obligated by October 30, 2026, with funds available for expenditure through September 2027. While the state has Sec. 71401 authority to spend, official notices caution that “Virginia has not yet opened formal Requests for Applications” for all sub-initiatives.
Instead, implementation partners are currently finalizing the statements of work and procurement frameworks necessary to release local RFAs. Initial local impacts are already emerging; for example, the Virginia Highlands Community College was awarded funding via the VCCS Foundation implementation partner to expand its LPN nursing track to clear local waitlists. Vendors and local entities are encouraged to join the official distribution list on the state’s Rural Health Transformation website to receive real-time alerts when RFAs are formally posted.
