
Alaska: LOI notifications drop ~May 29 as DOH runs back-to-back impact sessions on maternal health and chronic disease
Movement in Iowa, Alabama, Florida, and more

In this issue:
Iowa points to Iowa PCA for Communities of Care
Alabama first round of Notice of Funding Opportunities to be released on June 1. Sign up for roadshow stops
Florida adds link to HIE
Indiana RHTP Pre-Proposal Conference, May 20, 2026
Alaska: LOI notifications drop ~May 29 as DOH runs back-to-back impact sessions on maternal health and chronic disease
Nebraska updates their RFP timeline
Vermont adds five more RFPs
Iowa points to Iowa PCA for Communities of Care
An initiative that supports co-location of different rural provider types for convenient patient access and improved coordination, hires community health workers as system navigators, and invests heavily in chronic disease prevention and management techniques.
For more information on the technical assistance available for this effort, see our contracted TA provider's website.
From the PCA website:
The Iowa Primary Care Association (Iowa PCA) has been selected by the Iowa Department of Health and Human Services (Iowa HHS) to serve as the statewide Communities of Care Co-Location Technical Assistance Provider as part of Iowa’s Rural Health Transformation Program and the Healthy Hometowns initiative.
Alabama first round of Notice of Funding Opportunities to be released on June 1. Sign up for roadshow stops
ADECA is hosting workshops to provide an in-depth overview of the Alabama Rural Health Transformation Program (ARHTP) and the eleven initiatives developed for Alabama. See the memo below for more information: ARHTP Roadshow Workshop Announcements
Here’s the roadshow stops:
The Alabama Department of Economic and Community Affairs (ADECA) welcomes you to join us to learn more about the Centers for Medicare and Medicaid Systems’ Rural Health Transformation (RHT) Program and the eleven initiatives set forth by the State of Alabama to kick-start the goal of transforming health in Alabama’s rural communities.
These roadshow workshops will provide an in-depth overview of the RHT Program and the eleven initiatives developed for Alabama. Participants will have the opportunity to ask questions, gain valuable insights, and receive guidance to support application preparation ahead of the first round of Notice of Funding Opportunities, which will be released on June 1, 2026.
ADECA is committed to ensuring that every potential applicant has the resources, information, and support needed to fully understand the program and initiatives in order to successfully prepare and submit competitive applications.
May 26, 2026, 9:00-11:00 AM
Coastal Alabama Community College - Bay Minette Campus
2000 US-31, Bay Minette, AL 36507
Branch Building B - Room: 111
May 26, 2026, 5:30-7:30 PM
Troy University
100 University Avenue, Troy, AL 36082
Trojan Center - Lamar Higgins Ballroom
May 27, 2026, 9:00-11:00 AM
Gadsden State Community College
101 Padenreich Avenue, Gadsden, AL 35903
Advanced Manufacturing Flex Lab
May 27, 2026, 5:30-7:30 PM
University of North Alabama
649 Cramer Way, Florence, AL 35630
Wesleyan Auditorium
May 28, 2026, 9:00-11:00 AM
Alabama Center for Commerce
401 Adams Avenue, Montgomery, AL 36104
7th Floor Auditorium
The parking deck is located across the street at 400 Adams Avenue, and you can access the parking deck from the Decatur Street entrance by using the following code: 157865.
May 28, 2026, 5:30-7:30 PM
University of West Alabama
100 US-11, Livingston, AL 35470
Bell Conference Center
All individuals who will be attending a workshop must pre-register at https://app.smartsheet.com/b/form/019e3894425a749183762b4a22d9e523. The workshops are accessible to persons with disabilities. Persons with disabilities or special needs who may require special materials, services, or assistance should include this information in their registration.
Florida adds link to HIE
Rural Health Transformation Program (RHTP) - The Florida HIE
Discover how our products and services can transform data access and care coordination in your organization.
Here is how the Florida HIE specifically relates to the RHTP implementation:
Florida HIE/ENS Onboarding is a Key Initiative: One of the core initiatives driving the Technology & System Integration domain is explicitly named “Florida HIE/ENS Onboarding”. The Florida HIE is defined as the state’s platform for providing claims, encounter, and Event Notification System (ENS) analytics.
Measurable Interoperability Goals: The RHTP has a specific target to increase electronic health record (EHR) and diagnostic system interoperability adoption among rural health facilities by 10%. The goal is to move from a 2024 baseline of approximately 73% (236 out of 323 licensed hospitals connected to a national network) to at least 83% by Fiscal Year 2030.
Data-Driven Evaluation: The data generated from the Florida HIE will be actively used to evaluate the success of the RHTP. The External Evaluator hired by the state is required to design a data architecture capable of ingesting and synthesizing health information exchange and event notification data to track program performance over the five-year cooperative agreement.
Indiana RHTP Pre-Proposal Conference, May 20, 2026
Event Livestream Link
Event TimeEvent Name and LinkIGCS Conference Room9:30 am
The Rural Health Transformation Program (RHTP)
IGCS Conference Room 22
Alaska: LOI notifications drop ~May 29 as DOH runs back-to-back impact sessions on maternal health and chronic disease
Alaska published links to webinar recordings yesterday:
Healthy Beginnings RHTP Impacts Series: Session 2
Webinar Recording: Video Link
Presentation Slides/Materials: Resource Link
Healthy Communities RHTP Impacts Series: Session 2
Webinar Recording: Video Link
Presentation Slides/Materials: Resource Link
Here’s analysis
Commissioner Heidi Hedberg told two separate audiences on May 19, 2026 that Alaska’s RHTP Letter of Interest notifications go out at the end of next week — roughly May 29. The first time she said it was in the morning’s Impact Series #2 session on Healthy Beginnings (maternal health); the second was that same afternoon at Impact Series #3 on Chronic Disease and Self-Management with Dr. Ellen Hodges of Yukon-Kuskokwim Health Corporation as the featured guest.
Same phrasing both times: “Notices will be going out at the end of next week. Right now, we’re just populating it into the system to generate those notifications.” That’s the trigger that turns Alaska’s ~1,800 submitted LOIs into a real shortlist for the $272M Budget Period 1 award and tees up the first round of state-level RFPs.
Alaska DOH is running this public webinar series as the brokerage layer between vendors and Alaskan providers, organized by initiative track. Five impact sessions this week alone — Healthy Beginnings and Chronic Disease today, Healthcare Access tomorrow, Workforce on Friday.
133 people showed up to the maternal-health installment. Co-facilitators Dr. Anne Zink (now Yale SPH / Pew, formerly state CMO) and Dr. Lisa Rabinowitz (Providence Anchorage ED) explicitly framed it as a “dating session” — Alaskans and external vendors typing their names, orgs, and roles into the chat to find each other.
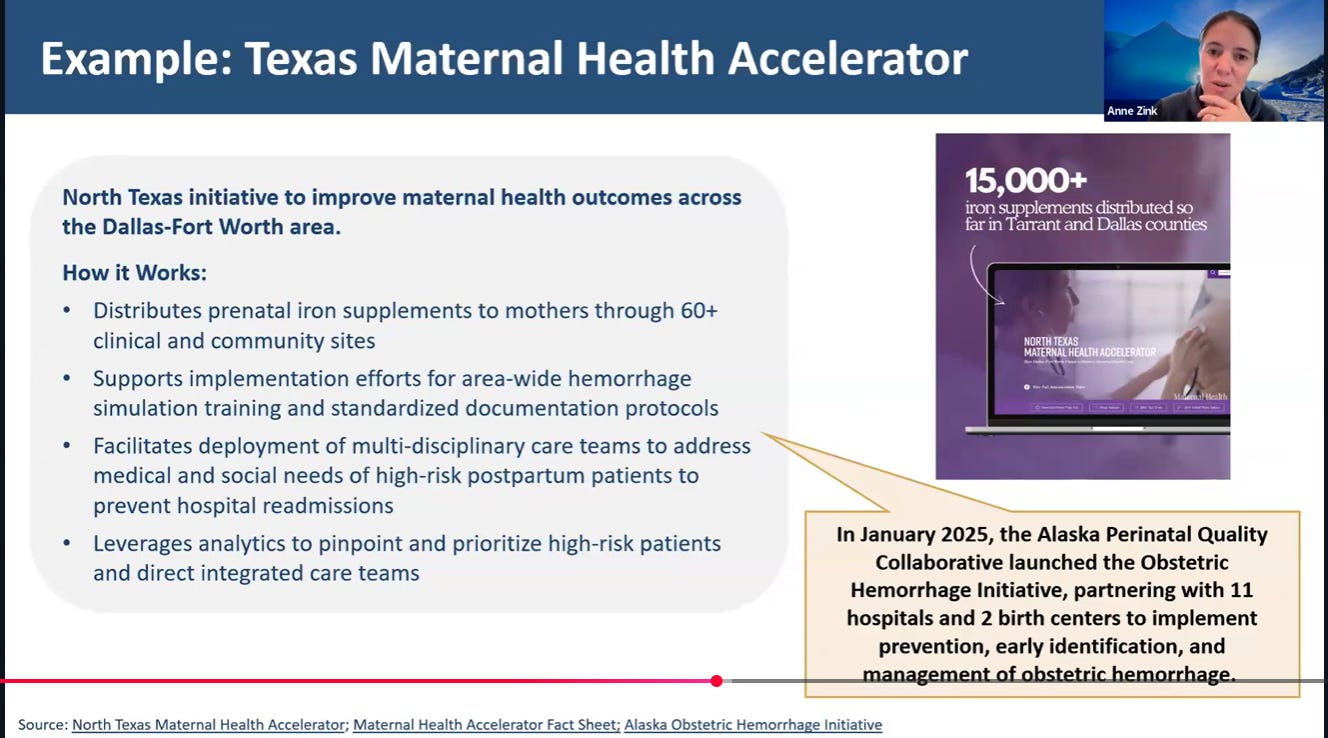
Maternal health: Texas-style insurer partnership as a sustainability play
The Impact Series #2 substance is built on a recognition that Alaska is losing ground on the maternal piece. Severe maternal morbidity and infant mortality both above national rates, 5 hospitals have dropped labor & delivery in the past 20 years, and most of the geography is more than 150 miles from an OB/GYN. One in 10 Alaska births already happens outside a hospital — three times the national average. The state’s response framework includes the Alaska Perinatal Quality Collaborative, the Substance Exposed Newborns initiative (4Ps Plus screening, state pays the license fee), home visiting via Nurse Family Partnership and Parents as Teachers, the Maternal Child Death Review Committee, and PRAMS/CUBS data systems — all under Becky Moresey, Section Chief for Women, Children & Family at AK DOH. Moresey openly asked the audience for visibility into who’s running maternal remote-patient-monitoring programs in the state — “we don’t really have good information” — a rare moment of program leadership admitting a market-map gap on a public call.
The model the facilitators kept holding up was the Texas Maternity Health Accelerator, specifically its payer-partnership angle: outcome gains translate into shared revenue back to the program, which is how Texas is making the work sustainable past the federal grant window. That’s a non-obvious bet for an RHTP state to surface this early — most are still optimizing for getting first-round dollars out the door, not for what happens at year five.
Chronic disease: YKHC’s playbook and a case-management gap
The afternoon session belonged to Dr. Ellen Hodges, YKHC Chief of Staff and a 23-year Y-K Delta family physician, who runs a tribal health system serving 56 tribes, 47 villages, and ~28,000 people across a roadless geography. Her framing of how to spend RHTP dollars was unambiguous: get care as close to home as possible, then strip out every barrier.
Her examples are the kind newsletter readers will remember — a mobile mammogram unit nicknamed “Sophie” that flies to sub-regional clinics in a small plane, a historical sub-regional colonoscopy program with a near-zero no-show rate, a YKHC Prescription Produce Program that ships culturally-relevant food boxes to villages, and a native-food donation program for shared subsistence harvests. Her one-liner of the session: “Make it as easy to use as TikTok.”
Dr. Sean Vanno, a 20-year Alaska family physician (Kodiak → Ketchikan → Bethel) described the tribal-vs-non-tribal integration gap with surgical clarity: tribal systems bundle diabetes, behavioral health, dental, optometry, and disease-specific case management into one organization, while non-tribal rural communities operate without that scaffolding.
His prescription: “Low-hanging fruit would be to develop case management for those areas that do not qualify for tribal health or federally qualified health.” That’s a concrete RHTP play hiding in plain sight — a state-funded case-management layer for the rural patients who aren’t already attached to a tribal or FQHC integrated system. 8 of Alaska’s top 12 causes of death are chronic diseases and only a quarter of Alaskans had a blood sugar test in the past three years — the LOI shortlist that drops next week will tell us whether the state’s $272M finds its way to that kind of upstream prevention work, or whether it gets absorbed into tertiary build-outs.
